What is an artificial heart?
An artificial heart is a prosthetic device that can take on the function of a human heart when necessary. The function of an artificial heart can be modeled as a process similar to those developed in chemical engineering applications. Several components of the human body serve as the process system that can be analysed when an artificial heart is used.
How does the natural human heart work?
Working to understand the various complex mechanisms and processes within the human body can potentially be useful in inciting innovation in biomedical fields. Because such systems are so intricate, it is necessary to pare down some of these and find ways to isolate them for individual study. It is also important to understand the functionality of the natural human heart, and how an artificial replacement works to mimic this functionality.
The natural human heart is controlled via a complex process involving a natural electrical system of sorts. The heart’s electrical system works to maintain a steady heart rate which varies to meet the body’s physical demand for oxygen at different levels of activity. With the help of conducting cells within the heart, which carry this electrical signal, and muscle cells, which allow for expansion and contraction of the heart, the heartbeat can be controlled.
Other processes within the human body also work to control the heartbeat. The brain, for instance, is integral in sending signals to the heart when a faster or slower heartbeat is necessary. The brain essentially works to control the initial electrical signal to the heart, which is fired off by the heart’s sinoatrial node. Hormones (i.e. adrenaline) and several components of the nervous system can also have a key impact in how the human body works to alter heart rate.
Approaching the design: how can an optimal artificial heart be developed?
The purpose of this journal is to design and study an artificial mechanical heart that can physically replace the natural human heart. Over the course of the past few years, both external and internal artificial hearts have been developed for people who have suffered chronic heart failure and have been ineligible for a total heart transplant. However, many of these artificial hearts, especially the earliest prototypes, have almost never been implanted successfully. Most prototypes have worked to produce a constant flow of blood throughout the human body. Only very recently have scientists began to develop more complicated control systems that change the output blood flow rate based on an increase in human activity (i.e. during periods of exercise). The design proposed in this journal works to control the oxygen concentration within blood by manipulating the blood flow rate and respiration rate.
Both an optimal material design and vigorous process control mechanism need to be considered in the development of the artificial heart proposed. Biocompatible materials are essential when designing a device to be implanted into the human body. In early artificial heart designs, plastic compounds and titanium were often used. In more recent design efforts, scientists have begun to incorporate biological components, i.e. valves made from chemically treated animal tissues.
Why does it need control?
In terms of process control, an artificial heart can serve to regulate the average oxygen concentration within the body. Depending on the user’s level of activity, physical condition, or human mass, the control system will help to manipulate the volumetric flow rate of blood being pumped throughout the body and the level of rate of oxygen intake. Signals are sent to the mechanical heart and to the brain in order to control these variables.
Maintaining the oxygen concentration in the blood within the body is vital to support human life. Nearly all of the body’s activities, from brain function to elimination, are regulated by oxygen. Oxidation is the essential factor for metabolic function, digestion, and circulation. Thus the proposed mechanical heart must be able to efficiently pump flow through the body, as well as be able to be manipulated by the controller to maintain healthy blood oxygen levels. Heart disease is considered a major health problem internationally. Fabricating a mechanical heart will allow people to live longer lives and maintain increased levels of activity.
The major protein that aids in the transport of oxygen in the blood is hemoglobin. In normal arteries, hemoglobin is about 97% saturated with oxygen. There are about 15 grams of hemoglobin per 100 mL of blood. Each gram of hemoglobin can bind to 1.34 mL of oxygen. Thus, the normal concentration of oxygen in arterial blood is 2.45*10^(-4) g/mL. According to the American Journal of Cardiology, blood concentration below 90% (or 2.27*10^(-4) g/mL) is considered to be potentially dangerous and is thus the lower limit of this operation.
How it works.
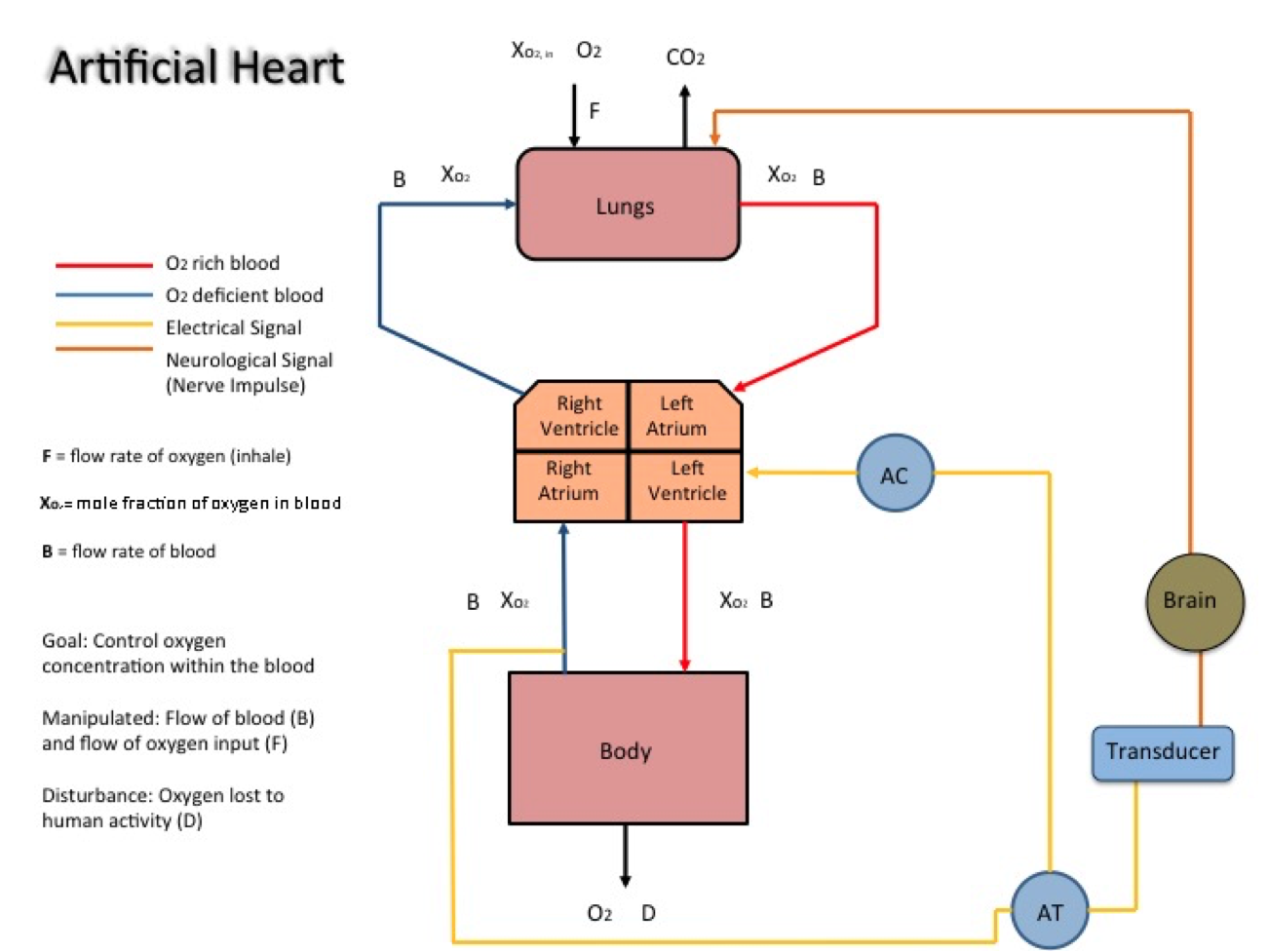
A concentration sensor-transmitter measures the remaining concentration of oxygen within blood after the blood cells deposit the oxygen throughout the body. This transmitter is located right before the right atrium in which the oxygen-depleted blood enters. The electrical signal is sent to two locations. First, it is sent to the proposed mechanical controller, which changes the speed of the artificial heartbeat via a pump. This action manipulates the flow of blood, thus controlling the amount of oxygen that can be delivered to the body. Additionally, the electrical signal is sent to a novel transducer, in which the signal can be transformed into a neurological impulse that is sent to the brain. The brain functions as a natural control system that changes the breathing pattern in the lungs. This manipulates the flow rate of air, thereby controlling the oxygen concentration within the blood.
The measured control variable, the oxygen concentration, changes upon disturbances such as an increased or decreased level of activity. The feedback process described above works eliminate rapid changes in oxygen concentration and to approach a set point.
One potential disturbance variable to consider in this process system is variation in human activity. Increased physical activity, such as cardiovascular exercise, will result in depletion of oxygen within the blood. The change in oxygen saturation will cause a deviation from the set point and theoretically, a feedback loop should cause the mechanical heart to pump at a faster rate to achieve the set point.
An artificial heart would be of great use to sufferers of heart disease and other related heart problems. Many biocompatibility issues would need to be addressed and studied before clinical use, which the blog post does address early on. The post also did well by emphasizing the importance of controlling oxygen concentration in the blood in order for implantation and use of an artificial heart to be successful, as opposed to simply being able to pump blood with the device. The post simplified the mechanisms of the control loop greatly; however, as a reader, I found this simplification helpful in order to gain the big picture of the control process. In addition, the schematic was helpful to visualize the feedback loop.
Feedback control makes sense for measuring the concentration of oxygen in the blood. Manipulating the flow of blood and intake air also makes sense in order to maintain the “healthy” concentration of oxygen. The signals sent to the brain and then to the lungs, seem like they would be harder to implement inside the human body because it requires the cooperation of organs and tissues already functioning inside the body. Whereas, the control of blood flow by a transmitter to a mechanical controller which then tells the mechanical heart to pump, seems to be easier to implement because all of the parts are being introduced into the body and working in the same loop together. I believe scientists and researchers in the future will be able to find a way for both mechanisms of control to be implemented inside the body. The heart, brain and lungs must work together for humans to survive; therefore, the use of an artificial heart must work in conjunction with the brain and lungs inside the body.
As the blog post stated, a change in human activity is a disturbance in the control system. The feedback control, as the post suggested, should be able to correct for the deviations in set point. If human activity increased, then more blood would need to be supplied to the body, which the feedback control as posited could correct for this disturbance. However, the design of the controller may want to account for an upper limit of oxygen concentration. I believe (research would be necessary to be absolutely sure) too much oxygen in the human body can cause complications; therefore, the controllers should have upper level parameters for oxygen concentration, so the artificial heart does not supply too much oxygen to the body, or the lungs do not take in oxygen too quickly, resulting in an over-supply of oxygen to the body.
The concept of engineering an artificial heart for use by sufferers of chronic heart diseases surely is an innovative one. Although the technology for implementing such an advanced system is far from being created, the potential benefits of this therapy is an immense one. The need for organ transplants is met with inadequate availability of resources and often leads to negative prognoses for the patients. This technology would prove to be some form of an upgraded pacemaker that can effectively regulate the cardiac rhythm through the detection of oxygen levels. One of the downsides to this however is the grueling surgery (which may be fatal) and recovery period that would follow a procedure to implant such a device into a human. This is because in this system, not only one but multiple vital organs are being targeted. In addition, the expertise of neurosurgeons, neurologists and cardio-thoracic surgeons to name a few will have to be enlisted. This of course will immensely drive up the cost of the procedure making it accessible to only a select few individuals who have the adequate resources or amazing medical insurance plans. Policy changes will also have to be implemented if this procedure is to be covered by medical insurance. I remain optimistic though that with the continuous advances in biotechnology and the discovery of biomaterials on the smaller scale will provide the necessary tools needed to engineer devices that are minimally invasive therefore mitigating the health risks stated earlier.
In terms of the mechanism of control to be used in this system, the idea of utilizing a simple feedback loop is a good start however due to the level of complexity involved with the human body, especially the cardiovascular and nervous systems, I would propose that a form of cascade control be utilized instead. It is required that the human body remain in a state of homeostasis. As such, the non-proactive characteristic of the feedback loop may prove to be fatal if there is a large deviation from the set-point due to other downstream processes. The secondary measurement points that are introduced with cascade control will recognize any changes in the blood oxygen concentration much sooner and help in the maintenance of homeostasis. Furthermore, as mentioned earlier, due to the need for stability within the human system a controller that is able to handle disturbances without compromising stability is desired. The type of controller action most able to do so would be a PID controller because of its ability to accurately reach the set-point without any offset and predict the response of the system from the responses that have been observed.
Finally, there should be safety measures in place to account for unfortunate occurrences such as a heart attack on one end or hyperventilation on the other. This should be accounted for in the robustness of the controller to be used. In an example scenario, when the heart stops all together, the flow of blood stops and oxygen concentration drops. The way this system is designed, there will still be signals going to the brain demanding more oxygen which will consequently exert more strain on the lungs. Such a situation could lead to irreversible organ damage and unfortunately, defeats the purpose of this mechanism all together. I think it would be of interest to explore potential safety measures to account for scenarios as I stated above.
The development of an artificial heart is important and helpful, as there has always been a shortage of organs donated for patients with heart failure. According to data provided by Organ Procurement and Transplantation Network, there are 4,144 candidates still on the waitlist for heart transplants as of April 8, 2016, and that is only the figure for America. Also, candidates for heart transplant is the third largest group among all organ transplant candidates, after kidney and liver organ groups. Therefore, it is vital that artificial heart technology is improved and eventually utilized to substitute for donor organ transplant. From the description by this blog, I think the artificial heart can be used by the general public, as significant progress has been made by introducing the control of oxygen concentration within the blood through varying blood flow rate instead of having a constant blood flow.
The control aspect of this newly designed artificial heart seems to be promising, as the concentration of oxygen within blood could be controlled to suit the needs of people with different level of needs (as people perform varying level of physical activities or are from different age/weight groups). This is a better controlled variable compared to, say, blood flow rate, as the level of oxygen in blood is the most essential factor for human well-being and blood is merely the carrier of oxygen. Depending on the concentration of oxygen in deoxygenated blood as detected by sensor-transmitter, blood flow rate and respiration rate are then manipulated for controlled variable to return to set-point.
As for disturbance variables, other than the variation of human activities, the altitude of the location that a person is in should also be factored into consideration. As the person goes to a place of a higher altitude, the concentration of oxygen in his or her surroundings decreases. Therefore, signals by the transmitter will demand an increase in blood flow rate and respiration rate in order to redress the set-point.
A PID controller should be used for the artificial heart. This is because a proportional-only control takes immediate corrective action when error is detected but offset (or steady-state error) occurs after a set-point change (for example, when the person performs a more strenuous physical activity and requires higher oxygen intake), and integral control should thus be used in conjunction to proportional control, as integral control eliminates offset but its control action only takes place until the error has persisted for some time. In addition, derivative control should be used because if there is a sharp change in disturbance variable, the controller should be able to pre-empt irreversible damage of organ failures.
There most certainly is a market for an artificial heart. There are so many people who need heart transplants or different devices implanted into their heart because of family history of heart disease or other reasons. Although there are different options out there, having an artificial heart that can measure the amount of oxygen in the blood and response accordingly is extremely beneficial. Different people have different levels active lifestyles. For some people, just walking up two flights of stair could be taxing. If the artificial heart was not able to measure and response to the amount of oxygen in the blood, this everyday task would be extremely difficult and dangerous those with the artificial heart.
The the control variable, the amount of oxygen in the blood, is important since, like they said, oxygen is needed in order for the body to work properly. It can be control using the manipulated variables, the flow rate of blood throughout the body and the respiration rate. The rate at which blood flows throughout the body is controlled by the pumping of the heart. The respiration rate is dependent on the lungs. Using these two things to control the oxygen concentration is very important. In addition to the activity level of the person with the artificial heart and their weight, size, height, and other unique characteristics, disturbance variables could also include the altitude at which the person is standing. At higher altitudes it is harder to breathe.
One control parameter that would be extremely important would be the time response. If someone is rapidly losing oxygen, you would want to control to act almost immediately to ensure that the oxygen level does not drop below the desired oxygen level. Unlike other processes, the consequences of reacting too slowly in this system are detrimental. The person could have permanent, irreversible damage or even death. In addition, you would not want to have a lot of overshoot because flushing the body with too much oxygen can also have negative consequences on the body. Because sometime the body does unpredictable things do the bacteria, viruses, and other sicknesses, I think it would be important to the controller to response to what it sees, what it has seen, and what it is going to see so a PID control should be used.