Arthrex Duplicate
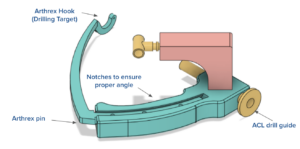
Our beta prototype includes two main subsystems, the ACLR FlipCutter® guide and the ALL arm extension. The ACLR FlipCutter® guide is heavily based on the Arthrex ACL RetroConstruction™ system as before, in order to efficiently adhere both to existing federal standards for these kinds of medical devices, as well as the preferences of our primary stakeholders. Dr. John Grant, an orthopedic surgeon we have been working closely with, recommended looking at Arthrex devices and drill guides specifically to get a better understanding of what modern surgeons are using. This subsystem has two parts, the handle and the angle arm. The handle is what the surgeon holds while operating the device, and it features a curved trapezoidal slot for the angle arm to slide in and out of (changing the trajectory of the drill), and a slot at the top for the 8mm drill to slot into. The handle also had the modification of cylindrical notches attached to the surface, which have grooves to allow the ALL arm extension to attach via set screw. The angle arm is what slides into the handle and is what actually mounts to the inside of the knee capsule, and as such is a highly specified, low-tolerance component. The side that slides into the handle has a constant radius in order to achieve that angle adjustability, while the side that slots into the knee tapers down to a curved point, complete with a sharp pin to hold it in place.
ALL Arm Extension
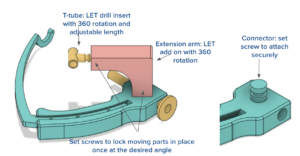
The ALL arm extension went through many iterations, beginning with a semi-arbitrarily-chosen geometry based on rough estimates of where the ALL drill trajectory would have to begin. It is in the shape of an L in order to begin at a location where it was deemed feasible to reach the general drilling location relative to the ACL tunnel. The 3-dimensional position of the ALL drill slot had to be both posterior and distal to the ACL drill slot, thus the L-shape to achieve these two distance adjustments. The arm extension slots onto the cylindrical notch (on either side, depending on the knee being operated on) and the angle it is rotated to will change the drill location in the coronal plane, which is controlled by the surgeon as they prepare an initial drilling trajectory. This arm extension also has a slot on the other end for a T-tube slider, which acts as the slot for the ALL drill and can rotate 360 degrees. This controls the drill location in the transverse plane of the femur (moving up or down on the horizontally-oriented bone). The angles of these components are set in place by tightening the respective set screws after the surgeon approximates the desired drill positions on the femur. With the current prototype, the device must be then taken out of the knee and then the drill bits must be inserted into the respective slots in order to check for tunnel convergence. However, the next step of the design is to add angle indicators on both the base of the arm extension and the T-tube ALL drill slot. In this way, a surgeon would only need to reference a number table to be informed of which angle combinations will result in tunnel convergence.
Our beta prototype, dubbed Mirage, follows a design philosophy more closely related to our Dune alpha prototype, which featured a 2-in-1 design having capabilities of drilling both the ACL and ALL tunnels. We chose to move forward with this design concept because it was the most fool-proof way of ensuring tunnel conflict avoidance since the tunnel trajectories can directly reference each other on one device. This sentiment was shared by both Dr. Grant, who we reconnected with after the conclusion of our alpha prototype phase, and our design review audience at Lafayette. Furthermore, according to Dr. Grant, our Oasis (or standalone) prototype allowed for too much variability through its skin-surface attachment method.
However, our Dune alpha prototype still had its own issues. While it served as a proof of concept that the general design philosophy was able to attain tunnel trajectories that avoided conflict, there was no failsafe mechanism that ensured such conflict avoidance. This is not ideal, since as Dr. Grant said, the main benefit of having a 2-in-1 guide is that there is the potential to set trajectories where the surgeon knows for certain that convergence will be avoided. The Dune prototype had no such failsafe mechanism. The crossbar feature also introduced too much variability since the T-tube component could slide freely along its entire length, so we resolved to eliminate this feature from our beta prototype design and instead create an ALL drill guide attachment that would directly mount onto the handle of the ACL FlipCutter® guide.
Codes and standards that were used in the creation of this device can be found here. These standards focus on the final stage of the design which is not where the team ended up. These codes and standards would be enforced once the device is fully completed and commissioned out of metal.